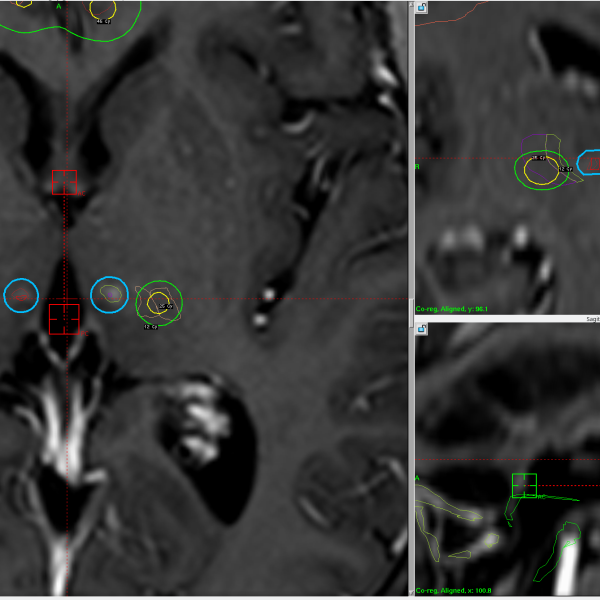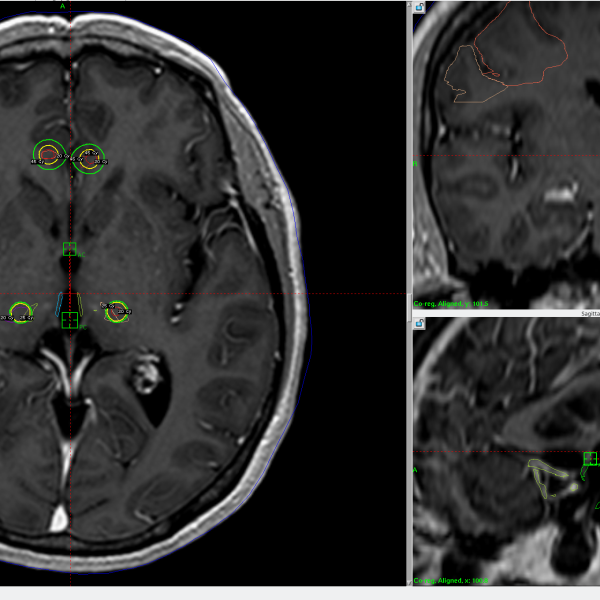
The Most Challenging Case Yet Phantom limb pain: Everything tried over the years at the local and peripheral levels has failed, including active treatment by algology and neuropsychology. Treatments have included an L2-L5 radiosurgical rhizotomy and—as you can see in the images—our most powerful approach: bilateral thalamotomy (120 Gy) and bilateral cingulotomy (90 Gy). We are one year out, and pain intensity is 8 to 10 out of 10.
What to do? This patient—as with so many out there—goes beyond the limits of what is known to medical science. Invasive alternatives are always available, such as attempts at DBS or cortical stimulation (rTMS has failed as well on her), but I believe—and the literature could demonstrate—that they are inferior or at least not superior to radiosurgery, in addition to this they are currently not available.
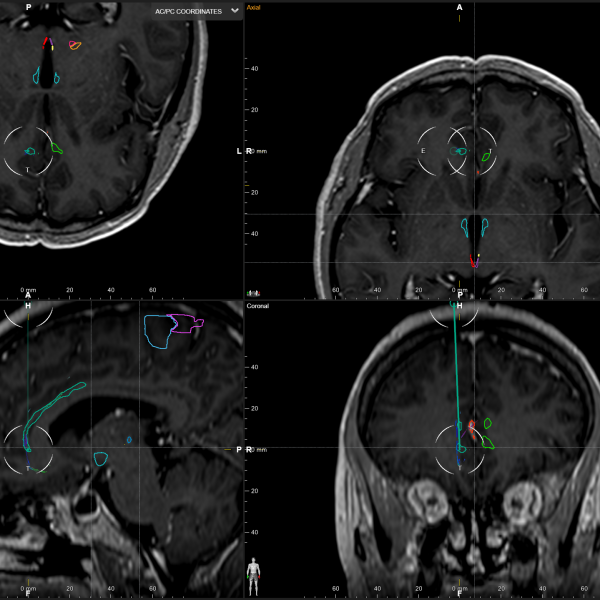
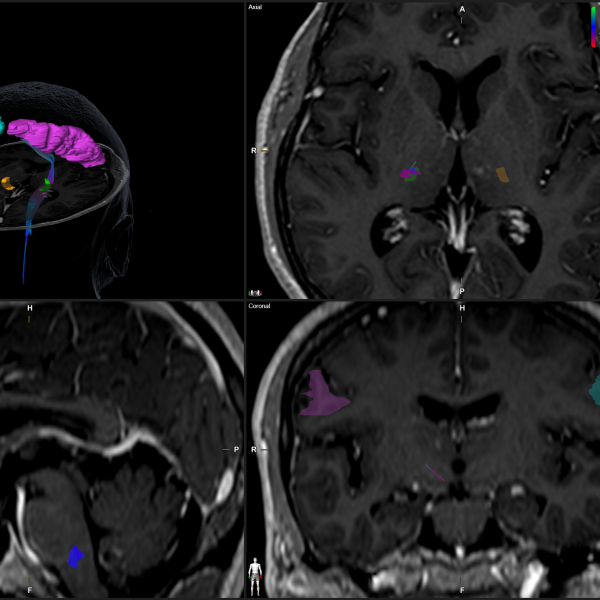
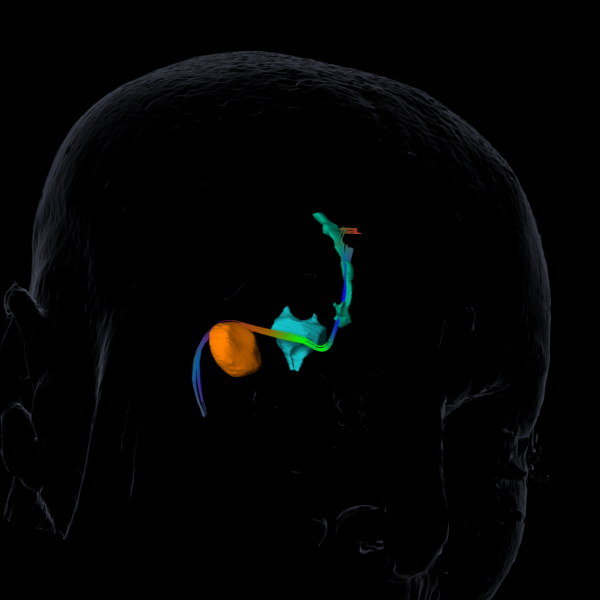
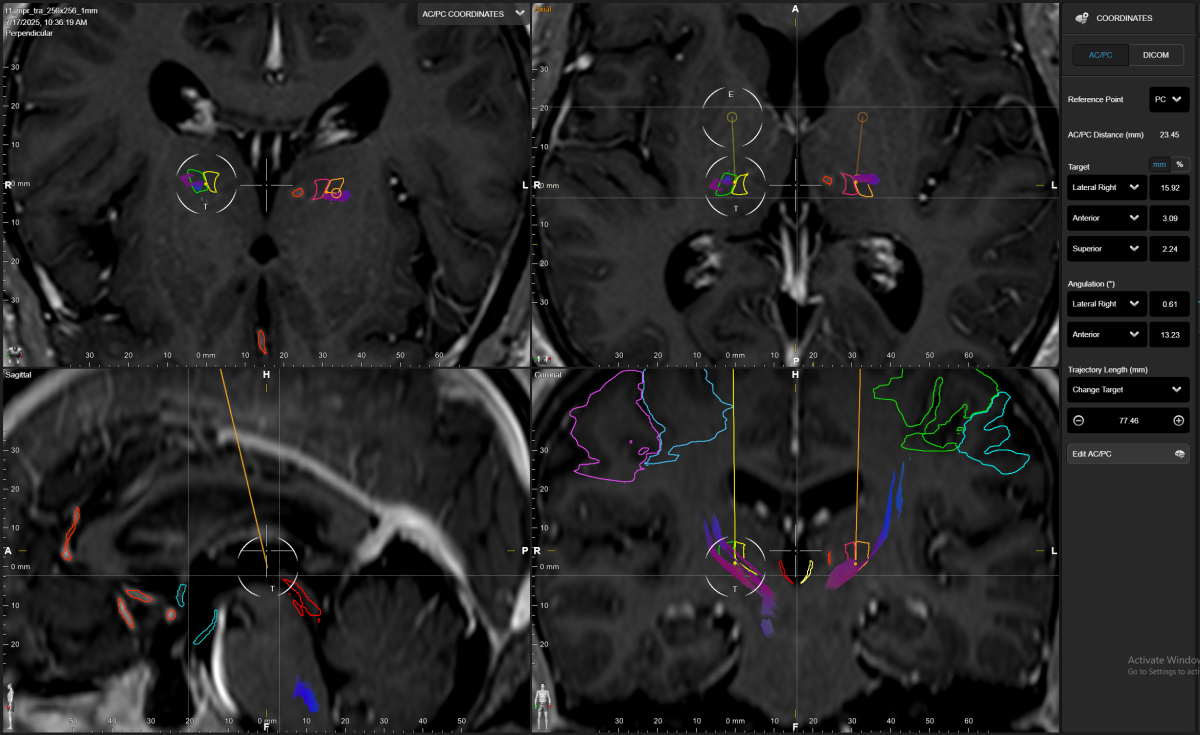
What’s new? Connectomic-based radiosurgery with Brianlab Elemnts. The approach is bilateral irradiation (50 Gy DMax) of the thalamus, but now to the VPL (previously, we used our classic CM-PFc target), and now a subgenual cingulotomy guided by connections to the hypothalamus and amygdala (90 Gy DMax).
What’s with the low doses? Recently, our published data showed how 90 Gy can be necrotic; this patient has contrast enhancement as well where we delivered 90 Gy to the right cingulum at a more traditional “surgical” targeting technique above the corpus callosum. 50 Gy might not be necrotic, but hopefully the 20 Gy isodose line can be modulatory, and this encompasses both the VPL and the VPM.
We shall keep our fingers crossed, hoping we can alleviate this wonderful lady. I'll keep you posted in the upcoming months.